Why eastern DRC’s peace efforts are vital to containing Ebola
Conflict, mistrust and closed borders are hindering the containment of Ebola in DRC and neighbouring countries.
Published on 23 June 2026 in
ISS Today
By
Rahel Hassen
Project Manager and Senior Researcher, East Africa, ISS Nairobi
Said Abdullahi
Research Intern, Conflict Prevention, Management, Resolution and Peacebuilding in the Great Lakes Region, ISS Nairobi
The deadly Bundibugyo strain of the Ebola virus has affected all three eastern Democratic Republic of the Congo (DRC) provinces – Ituri, North Kivu and South Kivu. By 22 June, there were 1 003 confirmed cases in the DRC and 19 in Uganda. Bundibugyo virus has an estimated fatality rate of 30%-50%, and there is no approved vaccine.
Health experts fear that delayed detection and access difficulties in eastern DRC mean the disease has been spreading for some time, creating uncertainty about infection numbers and geographical extent. In a region where healthcare was already weak, transmission is outpacing response capacity.
The outbreak is unfolding amid severe conflict in eastern DRC, which has prompted three peace processes: the Doha track which mediates between Kinshasa and M23, the Washington track aimed at reducing tensions between Kinshasa and Kigali, and the African Union (AU)-led process that complements the first two tracks.
These peace efforts matter not only for DRC’s stability but also for removing obstacles to the Ebola response, which suffers from three challenges: limited regional cooperation, community mistrust and conflict-induced restrictions on medical and humanitarian actors.
First, Ebola is a regional health and security threat, not only a national public health emergency. Containment requires coordinated action among officials from affected countries’ health departments and those working in foreign affairs and security, with national responses guided by World Health Organization (WHO) recommendations.
|
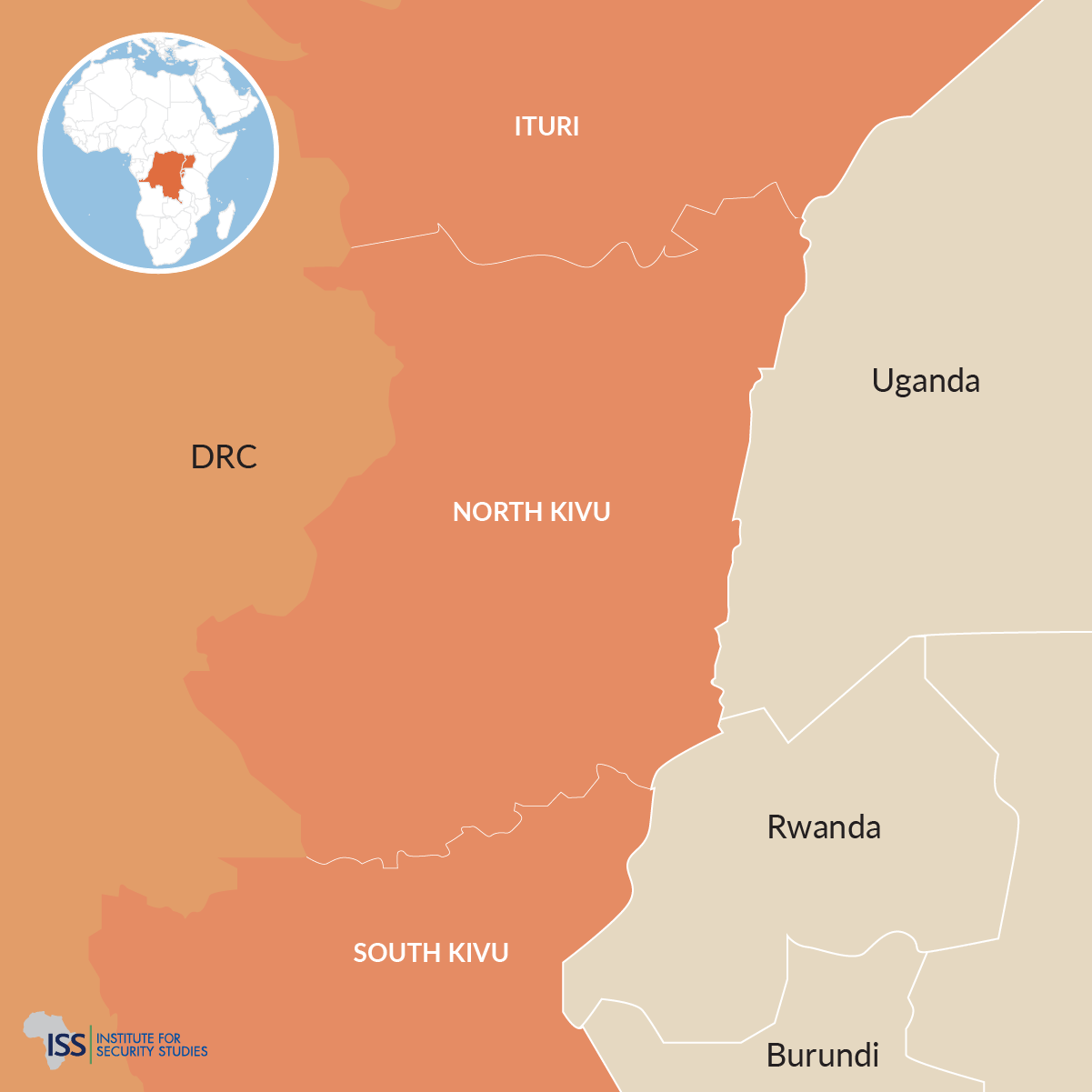
Eastern DRC and neighbouring countries
|
Coordination is particularly important in a region where cross-border communities link the DRC to its neighbours, Uganda, Rwanda and Burundi through a web of formal and informal crossing points. These connections limit authorities’ ability to monitor and regulate people’s movement. Cross-border mobility heightens Ebola transmission risks, as illustrated by cases linked to Congolese travellers entering Uganda.
Yet regional cooperation remains limited. Some neighbouring countries have instead opted for unilateral responses including border and airport closures. This goes against WHO recommendations, encourages informal border crossings and delays the movement of medical personnel, supplies and humanitarian assistance.
The limited cooperation is partly rooted in neighbouring countries’ competing economic and security interests in eastern DRC. Several countries are militarily involved and aligned with rival Congolese actors. This deepens mutual suspicion, as neighbours accuse one another of using armed groups as proxies. Inter-state rivalries and alliances make a coordinated regional response to the epidemic hard.
Inter-state rivalries and alliances make a coordinated regional response to the epidemic hard
The second challenge is community mistrust. In some cases, misinformation and beliefs that Ebola was introduced or prolonged for financial gain have fuelled attacks on health facilities and resistance to response teams. Flawed measures against the outbreak can also intensify mistrust. Response teams perceived as ethnically biased or dominated by non-local staff create openings for actors with vested interests to exploit local tensions.
Violence against health workers and facilities was already widespread before the current outbreak. Safeguarding Health in Conflict and Insecurity Insight documented at least 309 incidents of violence against or obstruction of health care in eastern DRC in 2025. This makes community engagement critical to effective Ebola management.
The third challenge is restricted access to affected communities and provision of supplies to Ebola-hit areas due to the ongoing conflict. In Ituri, the Ebola epicentre, attacks by the Allied Democratic Forces (ADF) and violence between communal armed groups disrupt movement, weaken public authority and threaten health facilities.
Armed groups expanded their influence when the DRC government redeployed its army from Ituri to Kivu to counter the M23 rebellion. North Kivu faces ADF attacks, and like Ituri, has been under martial law since 2021. In both North and South Kivu, fighting involving M23, the Congolese army and allied militias created multiple active frontlines and areas of contested control.
Responses to the Ebola outbreak require both protection measures and negotiated access
The outbreak coincides with a dire humanitarian situation that will probably deteriorate as Ebola-related restrictions are introduced. Armed actors, including the Congolese army and M23, continue to hamper humanitarian response efforts, restricting the movements of civilians and aid workers, and keeping critical infrastructures closed.
Responses to the outbreak require both protection measures and negotiated access. For non-cooperative armed groups such as the ADF, authorities have limited options beyond securing response corridors and protecting health workers and communities.
For armed groups more open to cooperation, negotiated access may be necessary, but politically risky. Such actors could use outbreak responses to claim legitimacy, consolidate control or secure access to resources.
These pressures are compounded by internal displacement. Conflicts displace people into overcrowded camps, which become areas of high Ebola transmission like the region’s dense mining settlements.
These conditions complicate surveillance, isolation, contact tracing and access to care. By creating a parallel trauma emergency, the conflicts force already overstretched health teams to split limited resources between outbreak control and conflict-related care.
The Doha, Washington and AU peace processes could all contribute to the containment of Ebola
Given the scale of the challenge and the DRC’s weak governance capacity, peace and stability should be integral to the outbreak response.
The three existing peace tracks could all contribute to Ebola containment. The Doha process could enable the DRC government and M23 to facilitate humanitarian access, cross-frontline referrals, disease surveillance and the movement of medical personnel and supplies. The ceasefire mechanism must be implemented because ending hostilities would facilitate cooperation on outbreak responses.
The Washington track could support DRC-Rwanda cooperation on border health measures, information sharing and the movement of suspected cases and contacts across national boundaries. The AU-led process could convene neighbouring states around a common regional response, including laboratory coordination, harmonised border measures and protection of humanitarian access.
Finally, community sensitisation about Ebola is vital. Delays could undermine the response to Ebola and complicate the implementation of peace agreements. Reduced violence and better cooperation would help contain the spread, while an uncontrolled outbreak could deepen instability and weaken fragile peace efforts.
For permission to re-publish ISS Today articles, please email us. In South Africa, News24 has exclusive rights to republish ISS Today articles. In Nigeria, Premium Times has exclusive rights to republish ISS Today articles.